
114@222
Brief summary of Solomon's opponent process theory
1) Body attempts to maintain
a physiologically stable milieu
2) Main goal is to minimize
deviations and maintain homeostasis
3) Any destabilizing disturbance triggers a
counterbalance, opponent, or compensatory maneuver. Tuesday, September 22,
4) Examples of such
destabilizing events would be any event that
disrupts affective or
emotional stability such as passion,
attachment, depression,
drugs (valium, cocaine, amphetamines,
alcohol etc.)
Primary reaction (a) to alcohol is mellow feeling, heightened sociability, and sedation but that
will soon be followed by the dreaded
hangover which consists of headaches, nausea, and
depression. This is the opponent after reaction. (b)
Amphetamine/cocaine primary response is euphoria,
well being, and self-confidence.(a) followed by fatigue and depression
(b).
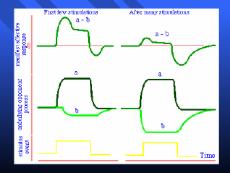
Solomon predicts that emotion
or drug tolerance is due to the interaction of a and b states where b subtracts
from a. A state (primary) > B
(opponent) after initial stimulation's but with repeated presentations of A
(primary) B intensifies and overshadows a state.
----------------------------------------------------------------------------
CR does not equal the UCR
More examples: laboratory
1) insulin >
hypoglycemia sac > in sac > in sac saline leads to hyperglycemia
2) epinephrine
(adrenaline) Sac > Pin (decrease in
gastric secretion Sac and saline
placebo (increase in gastric
secretion)/
page 2
3) Caffeine caffeine heart rate, decaf decrease
4) alcohol
UCR hypothermia; CR
hypothermia
4a) endorphins and why you
keep jogging
5) Siegel, Hinson, Krank
(1978)
Predrug signal in morphine
tolerance: support for Pavlovian conditioning
a) tolerance develops from
association between predrug stimuli environmental cues and the systemic effects
of the drug.
b) 2 x 2 x 2 groups of rats
administered morphine on 3 or 9 pairings, with complex environmental stimuli
paired or unpaired with saline or morphine.
Dependent variable analgesic
effect of the morphine
c) do not forget that
morphine cause decreased sensitivity to pain and this is what analgesia means.
d) conditioning model wins
out pain sensitivity greatest for the paired morphine contingent. Paw lick
sensitivity.
Tolerance or attenuated
analgesia is due to conditioning or to the systemic effects of the drug.
a. analgesia b. compensatory tolerance or increased
pain sensitivity.
Real life: rituals,
hypodermic, tourniquet, place, people, needle etc.
Pre Drug cues. Over trials
trigger b opponent state s\which is compensatory and pain sensitive.
Pre drug cues signal or
trigger opponent process which would by its very nature attenuate the drug's
effect. How to counter. Use different pre drug stimuli. Be leery of overdose.
Page 3
Anticipatory compensation
Morphine analgesic effect.
Method
CS visual auditory
UCS morphine
UCR analgesia or pain killing
CR depends on condition. Paired is counter-analgesic unpaired is
analgesic
2) tolerance development 2 x
2 x 2
3) tolerance testing paw
lick on hot plate
64 male rats
overhead room light fans
turned off =CS
Rats with pretest experience
with morphine in unpaired manner responded more slowly that paired morphine
groups and that is because the paired morphine group used the pre drug cues to
anticipate
compensatory responses
(counter analgesia) so when that hot plate was presented they were quick to
lick since the pain was greater for them relative to morphine unpaired, and
saline paired and unpaired.
The Risk of Heroin Overdose
Copied from p.56 (Box 5-1)
of 'Drugs and Behavior' by William A. McKim.
One of the greatest risks of
being a heroin addict is death from heroin overdose. Each year about
one percent of all heroin
addicts in the United States die from an overdose of heroin despite having
developed a fantastic
tolerance to the effects of the dr ug. In a nontolerant person the estimated
lethal dose of heroin may
range from 200 to 500 mg, but addicts have tolerated doses as high as
1800 mg without even being
sick[1]. No doubt, some overdoses are a result of mixing heroin with
other drugs, but appear to
result from a sudden loss of tolerance. Addicts have been killed one day
by a dose that was readily
tolerated the day before. An explanation for this sudden loss of tolerance
has been suggested by
Shepard Siegel of McMaster University, and his a ssociated, Riley Hinson,
Marvin Krank, and Jane
McCully.
Siegel reasoned that the
tolerance to heroin was partially conditioned to the environment where the
drug was normally
administered. If the drug is consumed in a new setting, much of the conditioned
tolerance will disappear and
the addict will be more likely to overdose. To test this theory Siegel and
associates ran the following
experiment[2].
Rats were given daily
intravenous injections for 30 days. The injections were either a dextrose
placebo or heroin and they
were given in either the animal colony or a different room where there
was a constant white noise.
The drug and the placebo
were given on alternate days and the drug condition always corresponded
with a particular
environment so that for some rats, the heroin was always administered in the
white
noise room and the placebo
was always given in the colony. For other rats the heroin ways given in
the colony and the placebo
was always given in the white noise room. Another group of rats served
as a control: these were
injected in different rooms on alternate dates, but were only injected with the
dextrose and had no
experience with the heroin at all.